
The term “chronic prostatitis” is very often used as a universal explanation for almost any genitourinary complaint in men. In some reports, the head of the infectious and inflammatory disease section of the European Association of Urology has referred to prostatitis as a “diagnostic wastebasket.”
Pain and discomfort in the perineum, urinary frequency, erectile problems, decreased libido, redness and rashes of the external genitalia are frequently and automatically attributed to prostate disease. However, from the perspective of evidence-based medicine, this approach is incorrect.
Prostatitis is not an age-related norm and does not occur in “almost all” men after the age of 30.
What is prostatitis from a medical standpoint?
Prostatitis is inflammation of the prostate gland. In the majority of cases, it is of bacterial origin.
According to the classification adopted by the European Association of Urology and the National Institutes of Health [1], the term “prostatitis” encompasses several distinct clinical entities.
Category I. Acute bacterial prostatitis [2]
A relatively rare but potentially severe condition. It is characterized by high fever (usually >37.5–38 °C), intense acute pain of a pressure-like or pulsating nature, marked deterioration of urination (hematuria, inability to void spontaneously, severe dysuria and burning), and significant impairment of general condition.
This condition requires urgent medical attention and prompt antibacterial therapy.
Category II. Chronic bacterial prostatitis [3]
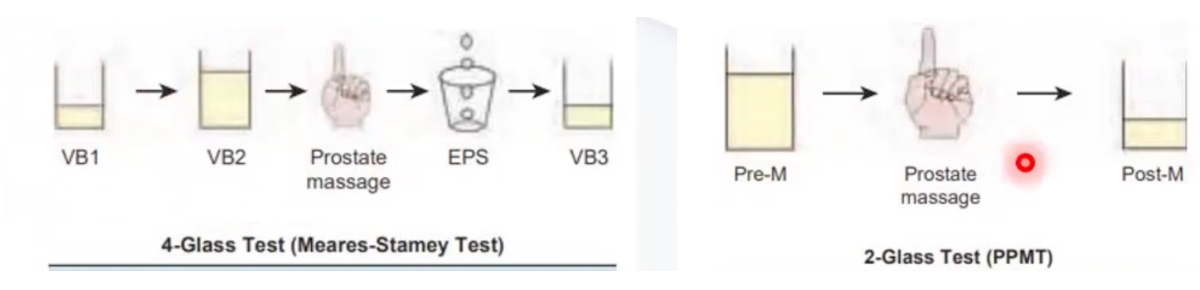
An uncommon condition. It is confirmed by evidence of inflammation in expressed prostatic secretion and/or in the two-glass (Nickel) or four-glass (Meares–Stamey) urine test [4], together with the presence of bacteria and recurrent urinary tract infections.
Category III. Chronic prostatitis / chronic pelvic pain syndrome (CPPS) [5,6]
Accounts for up to 90–95% of cases commonly labeled in everyday practice as “chronic prostatitis.” It is subdivided into inflammatory and non-inflammatory forms.
Key features include:
no identifiable infection,
laboratory tests often within normal limits,
lack of efficacy of antibiotics.
Category IV. Asymptomatic inflammatory prostatitis
Detected incidentally during examination, not accompanied by symptoms, and does not require treatment. It is often an incidental finding at autopsy and almost never influences clinical management.
Why is the diagnosis of “prostatitis” made so frequently?
In clinical practice, the term “prostatitis” is often used to describe any pelvic or urinary complaint, including:
- perineal discomfort,
- urinary frequency,
- weak urinary stream,
- sexual dysfunction,
- symptoms associated with stress or a sedentary lifestyle.
However, clinical guidelines emphasize that: the presence of symptoms does not equal prostate inflammation, and ultrasound findings alone are not diagnostic.
Why are antibiotics “just in case” not recommended?
According to the American Urological Association guidelines, in chronic pelvic pain syndrome:
- antibacterial therapy is not indicated, there is no evidence of its effectiveness,
- while the risk of adverse effects and antibiotic resistance remains high.
Antibiotics are justified only in cases of proven bacterial infection [7–9].
How do bacteria enter the prostate tissue?
Where do the symptoms come from, then?
The modern approach views chronic pelvic pain syndrome as a multifactorial condition. Contributing factors may include:
- pelvic floor muscle tension [10],
- altered pain perception [11,12],
- stress and anxiety disorders [11,12],
- prolonged sitting,
- sleep disturbances and chronic fatigue,
- and many other causes.
This does not mean that the symptoms are “imagined,” but they also cannot be reduced solely to inflammation or infection [13].
What do ultrasound and laboratory changes actually mean?
Findings such as:
- diffuse changes of the prostate, calcifications,
- mild prostate enlargement, are often misinterpreted.
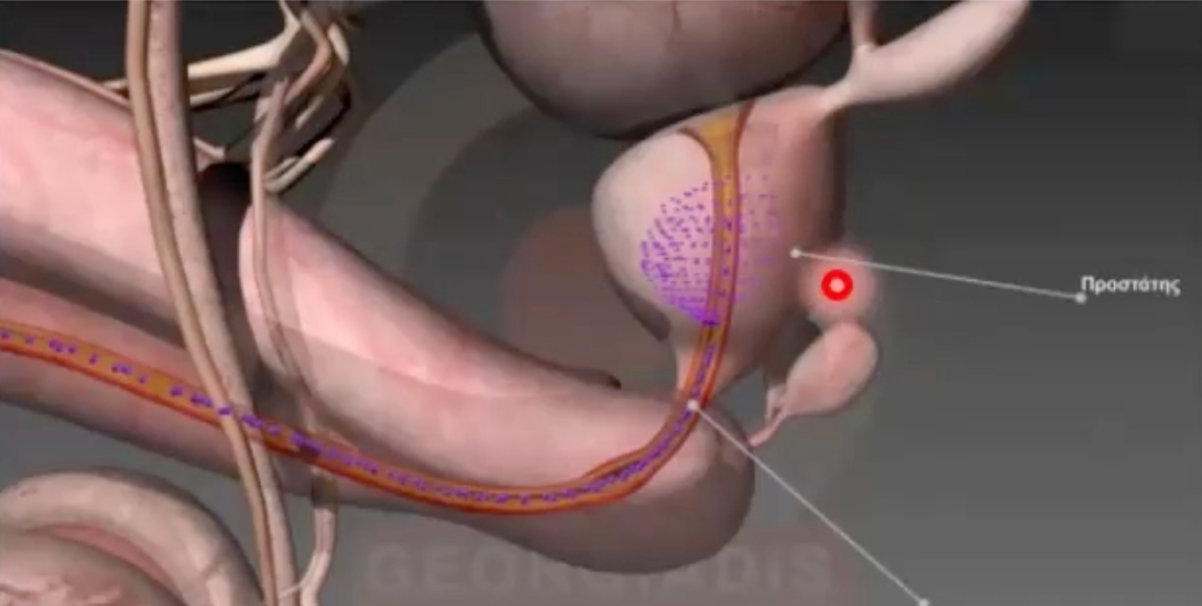
The formation of prostatic calculi/calcifications is associated with urethro-prostatic reflux—a condition in which urine refluxes through dilated prostatic ducts deep into the acini of the prostate. This occurs when intravesical pressure increases and the bladder neck allows urine to pass into the prostatic urethra. Part of the urine penetrates the prostate tissue, causing chemical irritation, followed by aseptic (non-bacterial) inflammation, and ultimately calcification of the damaged area.
It is also important to note that ultrasound alone is not required to establish a diagnosis of prostatitis, as it cannot confirm the presence of bacteria or active inflammation. Ultrasound is used primarily to exclude complications of true prostatitis and should be performed strictly based on clinical indications.

It is crucial to understand that prostatitis is not an inevitable age-related diagnosis. A thorough and competent evaluation by a urologist experienced in pelvic disorders is of paramount importance in order to exclude other causes of pain and discomfort.
Most cases of chronic symptoms are not associated with infection. Antibiotics are rarely indicated and only in the presence of a proven bacterial cause. Treatment should be individualized and multimodal. Self-medication and overtreatment more often worsen the condition than improve it.
Действительно ли есть хронический простатит у каждого мужчины после 30?
Термин «хронический простатит» очень часто используется как универсальное объяснение любых жалоб со стороны мочеполовой системы у мужчин. В некоторых докладах глава Европейской ассоциации урологов по контролю и лечения инфекционно-воспалительных заболеваний называл простатит “ мусорной корзиной из диагнозов”. Боли и дискомфорт в промежности, учащённое мочеиспускание, проблемы с эрекцией, снижение либидо, покраснения и высыпания на наружных половых органах нередко автоматически связывают с заболеванием предстательной железы. Однако с точки зрения доказательной медицины такой подход неверен.
Простатит не является возрастной нормой и не встречается «почти у всех» мужчин после 30 лет.
Что такое простатит с медицинской точки зрения?
Простатит- воспаление предстательной железы. В превалирующем числе случаев - бактериальной природы.
Согласно классификации, принятой European Association of Urology и National Institutes of Health [1] , под термином «простатит» понимается несколько разных состояний.
I класс.Острый бактериальный простатит [2]
На самом деле редкое, но достаточно серьёзное заболевание. Характеризуется высокой температурой ( более 37,5-38С), выраженной острой болью распирающего/ пульсирующего характера, значительным ухудшением мочеиспускания ( примесь крови, невозможность самостоятельного мочеиспускания, рези и жжение), нарушением общего состояния. Требует срочного медицинского вмешательства и антибактериальной терапии.
II класс. Хронический бактериальный простатит [3]
Встречается редко. Подтверждается наличием воспаления в секрете простаты/ двустаканной ( Nickel) или четырехстаканной пробе мочи ( Mearsy- Stamey) [4], а также бактерий и рецидивирующими инфекциями мочевых путей.
III класс. Хронический простатит / синдром хронической тазовой боли (CPPS) [5,6]
Составляет до 90–95% всех случаев, которые в быту называют «хроническим простатитом». Подразделяется на 2 класса: воспалительный и невоспалительный.
При этом:
• инфекция не выявляется,
• анализы часто находятся в пределах нормы,
• антибиотики неэффективны.
IV класс. Бессимптомное воспаление простаты
Выявляется случайно при обследовании, не сопровождается жалобами и не требует лечения. Очень часто является находкой после смерти и почти никогда не влияет на тактику ведения пациента.
Почему диагноз «простатит» ставят так часто?
На практике словом «простатит» нередко обозначают любые жалобы в области таза и мочеиспускания, в том числе:
• дискомфорт в промежности,
• учащённые позывы к мочеиспусканию,
• ослабление струи мочи,
• сексуальные нарушения,
• симптомы на фоне стресса или малоподвижного образа жизни.
Тем не менее, клинические рекомендации подчёркивают:
наличие симптомов не означает воспаление простаты, а изменения на УЗИ не являются диагнозом
Почему антибиотики «на всякий случай» не рекомендованы?
Согласно рекомендациям American Urological Association, при синдроме хронической тазовой боли:
• антибактериальная терапия не показана,
• доказательств её эффективности нет,
• при этом риск побочных эффектов и антибиотикорезистентности остаётся высоким.
Назначение антибиотиков допустимо только при подтверждённой бактериальной инфекции [7-9].
Механизм попадания бактерий в ткань предстательной железы
Откуда тогда берутся симптомы?
Современный подход рассматривает синдром хронической тазовой боли как многофакторное состояние. В развитии симптомов могут участвовать:
• мышечное напряжение тазового дна, [10]
• нарушения болевой чувствительности[11,12],
• стресс и тревожные расстройства [11,12],
• длительное сидение,
• нарушения сна и хроническое переутомление
• и очень много других причин
Это не означает, что симптомы «надуманы», но и не сводится к воспалению или инфекции [13]
Что означают изменения на УЗИ и в анализах?
Такие находки, как:
• диффузные изменения простаты,
• кальцинаты,
• умеренное увеличение железы
Причиной возникновения конкрементов/ кальцинатов/камней в простате является уретро-простатический рефлюкс — состояние при котором возникает заброс мочи по расширенным протокам простаты в глубь ацинусов предстательной железы. Он возникает по причине того, что давление в мочевом пузыре возрастает и шейка мочевого пузыря начинает пропускать мочу в простатический отдел уретры. Часть мочи проникает в ткань предстательной железы вызывая в ней химический ожог, далее возникает асептическое ( небактериальное) воспаление, и в итоге поврежденный участок простаты — кальцифицируется.
Также важным уточнением является то, что для установки диагноза “простатит” УЗИ само по себе не требуется, так как не может подтвердить наличие бактерий или воспаления. По УЗИ мы можем исключить наличие осложнений “истинного простатита” и оно выполняется строго по
показаниям
Таким образом, важно понимать, что простатит не является обязательным возрастным диагнозом. Колоссальное значение имеет грамотный осмотр врача-уролога, который специализируется на “тазовых заболеваниях” и может исключить другие причины боли и дискомфорта. Большинство случаев хронических симптомов не связаны с инфекцией. Антибиотики показаны редко и только при доказанной бактериальной причине. Лечение должно быть индивидуальным и комплексным. Самолечение и избыточная терапия чаще ухудшают ситуацию, чем помогают.
[1] Krieger JN, Nyberg L, Nickel JC: NIH consensus definition and classification of prostatitis. JAMA 282:236–237, 1999.
[2] Alexander, R.B., et al. Elevated levels of proinflammatory cytokines in the semen of patients with chronic prostatitis/chronic pelvic pain syndrome. Urology, 1998. 52: 744.
[3] Alexander, R.B., et al. Chronic prostatitis: results of an Internet survey. Urology, 1996. 48: 568.
[4] Meares, E.M., et al. Bacteriologic localization patterns in bacterial prostatitis and urethritis. Invest Urol, 1968. 5: 492.
[5] Zermann, D.H., et al. Neurourological insights into the etiology of genitourinary pain in men. J Urol, 1999. 161: 903.
[6] Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet, 2015. 386: 743.
[7] Lai HH, Pontari MA, Argoff CE, et al. Male Chronic Pelvic Pain: AUA Guideline: Part I Evaluation and Management Approach. J Urol. 0(0). doi:10.1097/JU.0000000000004564. https://www.auajournals.org/doi/10.1097/JU.0000000000004564
[8] Lai HH, Pontari MA, Argoff CE, et al. Male Chronic Pelvic Pain: AUA Guideline: Part II Treatment of Chronic Prostatitis/Chronic Pelvic Pain Syndrome. J Urol. 0(0). doi:10.1097/JU.0000000000004565. https://www.auajournals.org/doi/10.1097/JU.0000000000004565
[9] Lai HH, Pontari MA, Argoff CE, at al. Male Chronic Pelvic Pain: AUA Guideline: Part III Treatment of Chronic Scrotal Content Pain. J Urol. 0(0). doi:10.1097/JU.0000000000004566. https://www.auajournals.org/doi/10.1097/JU.0000000000004566
[10]Slocumb, J.C. Neurological factors in chronic pelvic pain: trigger points and the abdominal pelvic pain syndrome. Am J Obstet Gynecol, 1984. 149: 536.
https://www.ncbi.nlm.nih.gov/pubmed/6234807
https://www.ncbi.nlm.nih.gov/pubmed/26063472
[11] Melzack, R., et al. Central neuroplasticity and pathological pain. Ann N Y Acad Sci, 2001. 933: 157.
https://www.ncbi.nlm.nih.gov/pubmed/12000018
[12] Fulbright, R.K., et al. Functional MR imaging of regional brain activation associated with the affective experience of pain. AJR Am J Roentgenol, 2001. 177: 1205.
https://www.ncbi.nlm.nih.gov/pubmed/11641204
[13] Nickel, J.C., et al. Chronic Prostate Inflammation Predicts Symptom Progression in Patients with Chronic Prostatitis/Chronic Pelvic Pain. J Urol, 2017. 198: 122.
https://www.ncbi.nlm.nih.gov/pubmed/28089730