Erectile dysfunction (ED) is a condition in which a man regularly has difficulty achieving or maintaining an erection sufficient for satisfactory sexual activity [1]. This is not only an intimate issue — ED can seriously affect emotional well-being, self-confidence, relationships, and overall quality of life for a man and his partner [2]. Nowadays, it is known that the causes of ED are almost never “purely psychological” or “purely physiological.” It is usually a combination of factors — which is why terms such as “predominantly organic” or “predominantly psychogenic” ED are increasingly used.
Epidemiological data show high prevalence and incidence of erectile dysfunction worldwide [3]. For example, the Massachusetts Male Aging Study (MMAS) demonstrated an overall ED prevalence of 52% among men aged 40–70 living in the Boston area. The rates of minimal, moderate, and complete ED were 17.2%, 25.2%, and 9.6%, respectively.
In the Cologne study among men aged 30–80, the prevalence of ED was 19.2%, with a sharp age-related increase — from 2.3% to 53.4% [4]. In another study of men seeking medical help for newly developed ED, one in four patients was younger than 40, and nearly 50% of them reported severe sexual dysfunction.*
Why Is Erectile Dysfunction an Important Integral Indicator of Health?
An erection is a complex physiological process that involves blood vessels, nerves, hormones, and the brain. Problems may arise due to various diseases and levels of dysfunction: vascular (including atherosclerosis), hormonal disorders, neurological diseases, chronic stress, or anxiety [5].
From the standpoint of urological health, ED may result from a wide range of conditions, including lower urinary tract symptoms and benign prostatic hyperplasia, chronic pelvic pain syndrome (CPPS) and chronic prostatitis [6], bladder pain syndrome/interstitial cystitis [7], premature ejaculation [8], and surgical correction of posterior urethral strictures.
Men seeking medical help for erectile difficulties often have hidden or newly diagnosed cardiovascular disease (CVD). Studies show that ED significantly increases the risk of coronary artery disease, stroke, atrial fibrillation, as well as cardiovascular mortality and all-cause mortality [9]. Importantly, even temporary erectile problems in men under 50 may be an early sign of elevated cardiovascular risk [10].
This means ED is often the earliest predictor of cardiovascular disease — often before chest pain occurs or ECG abnormalities appear. More severe and long-lasting ED typically indicates a higher cardiovascular risk, and ED itself increases the accuracy of screening for hidden CVD [11].
The Princeton Consensus Conference series has focused on how to most effectively and safely assess and treat men with ED and potential cardiovascular risks [12]. Modern European guidelines for ED (EAU) are based on the latest Princeton Consensus version published in 2024 [13].
The fourth Princeton Consensus revised the algorithms for cardiovascular risk assessment in men with ED and recommended using the ASCVD score (American College of Cardiology/American Heart Association) to estimate the 10-year risk of major cardiovascular events [14]. This calculation considers age, sex, cholesterol levels, blood pressure, smoking, and diabetes after consultation with a cardiologist.
Updated Princeton algorithms help the physician determine:
- whether sexual activity is safe in the presence of CVD;
- whether advanced cardiac screening is required;
- whether PDE-5 inhibitors (e.g., sildenafil) can be prescribed, especially if the patient occasionally uses nitrates.
Erectile Dysfunction and Mental Health: When Emotions Affect the Body
Mental health problems often accompany erectile dysfunction [15]. The most common psychological factors include depression and anxiety disorders, but temporary emotional crises — work-related stress, family conflicts, loss, and exhaustion — are also frequent contributors [16,17].
The emotional atmosphere of a relationship plays a major role. Dissatisfaction with the partnership, reduced sexual harmony, long relationship duration, and lack of emotional closeness during sex all increase the risk of developing ED. Conversely, trust and emotional support from a partner act as protective factors: men who feel emotionally safe in their relationships are much less likely to experience severe erection problems [16].
When the Cause Is Not Physical
Psychogenic erectile dysfunction is a form of ED caused mainly by psychological factors while physiological mechanisms remain intact.
Unlike organic ED, psychogenic ED usually allows a man to maintain an erection in situations where sexual intercourse is not expected or possible [17].
Typical features include:
- erectile difficulties only with certain partners or in specific circumstances;
- preserved erections during sleep or masturbation;
- sudden onset of symptoms after a period of normal sexual function.
These characteristics allow the physician to infer that the primary cause lies in the emotional sphere [18,19].
Performance Anxiety Syndrome
One of the key psychological mechanisms sustaining ED is performance anxiety syndrome. After one negative sexual experience, a man becomes anxious before intercourse, increasing tension and reducing the quality of his erection.
Typical manifestations include:
- fear of premature ejaculation;
- worry about being unable to achieve orgasm;
- fear of losing the erection during intimacy.
This anxiety creates a vicious cycle: the stronger the fear of failure, the higher the likelihood of its recurrence.
Why Is Psychosexual Assessment Important?
Even in “organic” ED (e.g., due to vascular disease or medication side effects), cognitive and emotional factors are often involved.
Negative beliefs, excessive self-monitoring, low self-esteem, or distraction from erotic stimuli can significantly worsen erectile difficulties.
Therefore, assessing both physical and psychological health is essential.
Psychosexual assessment typically includes:
- a consultation discussing emotions, relationships, stress levels, and sexual expectations;
- when needed, standardized psychological questionnaires that help objectively evaluate anxiety, depression, and emotional tension.
The Multifaceted Nature of Erectile Dysfunction
Erectile dysfunction almost never has a single cause. A patient may simultaneously have vascular, hormonal, and neurological issues, medication effects, stress, and relationship problems [20].
For this reason, ED is now viewed as an integral indicator of men’s health, reflecting both physical and psychological well-being.
Effective treatment requires a comprehensive approach involving a urologist, cardiologist, psychotherapist, and, when necessary, an endocrinologist.
The most important thing to remember: even in cases of severe ED, erectile function often improves significantly with timely professional help.
- NIH, C.D.P.o.I. NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA, 1993. 270: 83.
- - Feldman, H.A., et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol, 1994. 151: 54. -Fisher, W.A., et al. Erectile dysfunction (ED) is a shared sexual concern of couples I: couple conceptions of ED. J Sex Med, 2009. 6: 2746. -Salonia, A., et al. Is erectile dysfunction a reliable proxy of general male health status? The case for the International Index of Erectile Function-Erectile Function domain. J Sex Med, 2012. 9: 2708.- Corona, G., et al. Assessment of the relational factor in male patients consulting for sexual dysfunction: the concept of couple sexual dysfunction. J Androl, 2006. 27: 795.
- -Feldman, H.A., et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol, 1994. 151: 54.
- -Braun, M., et al. Epidemiology of erectile dysfunction: results of the 'Cologne Male Survey'. Int J Impot Res, 2000. 12: 305.
- -Wright, L.N., et al. Erectile Dysfunction and Treatment: An Analysis of Associated Chronic Health Conditions. Urology, 2021. 157: 148.
- Li, H.J., et al. Prevalence of sexual dysfunction in men with chronic prostatitis/chronic pelvic pain syndrome: a meta-analysis. World J Urol, 2016. 34: 1009.
- Chung, S.D., et al. A nationwide population-based study on bladder pain syndrome/interstitial cystitis and ED. Int J Impot Res, 2013. 25: 224.
- .van der Poel, H.G., et al. Focal Therapy in Primary Localised Prostate Cancer: The European Association of Urology Position in 2018. Eur Urol, 2018. 74: 84.
- - Tanaka, Y., et al. Association of Erectile Dysfunction with Incident Atrial Fibrillation: The Multi-Ethnic Study of Atherosclerosis (MESA). Am J Med, 2020. 133: 613.
- Fang, S.C., et al. Changes in erectile dysfunction over time in relation to Framingham cardiovascular risk in the Boston Area Community Health (BACH) Survey. J Sex Med, 2015. 12: 100.
- Adam, A., et al. Is the History of Erectile Dysfunction a Reliable Risk Factor for New Onset Acute Myocardial Infarction? A Systematic Review and Meta-Analysis. Curr Urol, 2020. 14: 122.
- Rosen, R.C., et al. Proceedings of PRINCETON IV: PDE5 inhibitors and cardiac health symposium. Sex Med Rev, 2024. 12: 681.
- Kloner, R.A., et al. Princeton IV consensus guidelines: PDE5 inhibitors and cardiac health. J Sex Med, 2024. 21: 90.
- Reiter-Brennan, C., et al. ACC/AHA lipid guidelines: Personalized care to prevent cardiovascular disease. Cleve Clin J Med, 2020. 87: 231.
- Li, K., et al. The Relationships of Dehydroepiandrosterone Sulfate, Erectile Function and General Psychological Health. Sex Med, 2021. 9: 100386.
- Liu, Q., et al. Erectile Dysfunction and Depression: A Systematic Review and Meta-Analysis. J Sex Med, 2018. 15: 1073.
- Rosen, R.C., et al. Men with Sexual Problems and Their Partners: Findings from the International Survey of Relationships. Arch Sex Behav, 2016. 45: 159.
- Sivaratnam, L., et al. Behavior-Related Erectile Dysfunction: A Systematic Review and Meta-Analysis. J Sex Med, 2021. 18: 121.
- Brotto, L., et al. Psychological and Interpersonal Dimensions of Sexual Function and Dysfunction. J Sex Med, 2016. 13: 538.
- Parent, M.C., et al. Heterosexual Self-Presentation, Identity Management, and Sexual Functioning Among Men Who Have Sex with Men. Arch Sex Behav, 2021. 50: 3155.
Эректильная дисфункция (ЭД) — это состояние, при котором мужчине регулярно трудно получить или удержать эрекцию, достаточную для полноценного сексуального контакта [1]. Это не только интимная проблема — эректильная дисфункция способна серьезно влиять на эмоциональное состояние, уверенность в себе, отношения и общее качество жизни мужчины и его партнёрши [2]. В настоящее время известно, что причины ЭД почти никогда не бывают «чисто психологическими» или «чисто физиологическими». Обычно это сочетание факторов — поэтому всё чаще используют понятия «преимущественно органическая» или «преимущественно психогенная» ЭД.
Эпидемиологические данные показывают высокую распространенность и заболеваемость эректильной дисфункцией (ЭД) во всём мире [3]. В частности, исследование Massachusetts Male Aging Study (MMAS) продемонстрировало общую распространенность ЭД на уровне 52% среди мужчин 40–70 лет, проживающих в районе Бостона. При этом частота минимальной, умеренной и полной ЭД составила 17,2%, 25,2% и 9,6% соответственно. В Кёльнском исследовании среди мужчин 30–80 лет распространенность ЭД составила 19,2%, причём отмечался резкий рост с возрастом — от 2,3% до 53,4% [4]. В одном из исследований, включающем мужчин, впервые обратившихся за медицинской помощью по поводу недавно возникшей ЭД, оказалось, что каждый четвертый пациент был младше 40 лет, и почти 50% из них жаловались на тяжелую степень сексуальной дисфункции*
Почему эректильная дисфункция является важным интегральным показателем здоровья?
Эрекция — сложный физиологический процесс, в котором работают сосуды, нервы, гормоны и головной мозг. Нарушения могут появляться на фоне разных заболеваний и уровней поражения: сосудистых (включая атеросклероз), гормональных нарушений, болезней нервной системы, хронического стресса или тревоги [5].
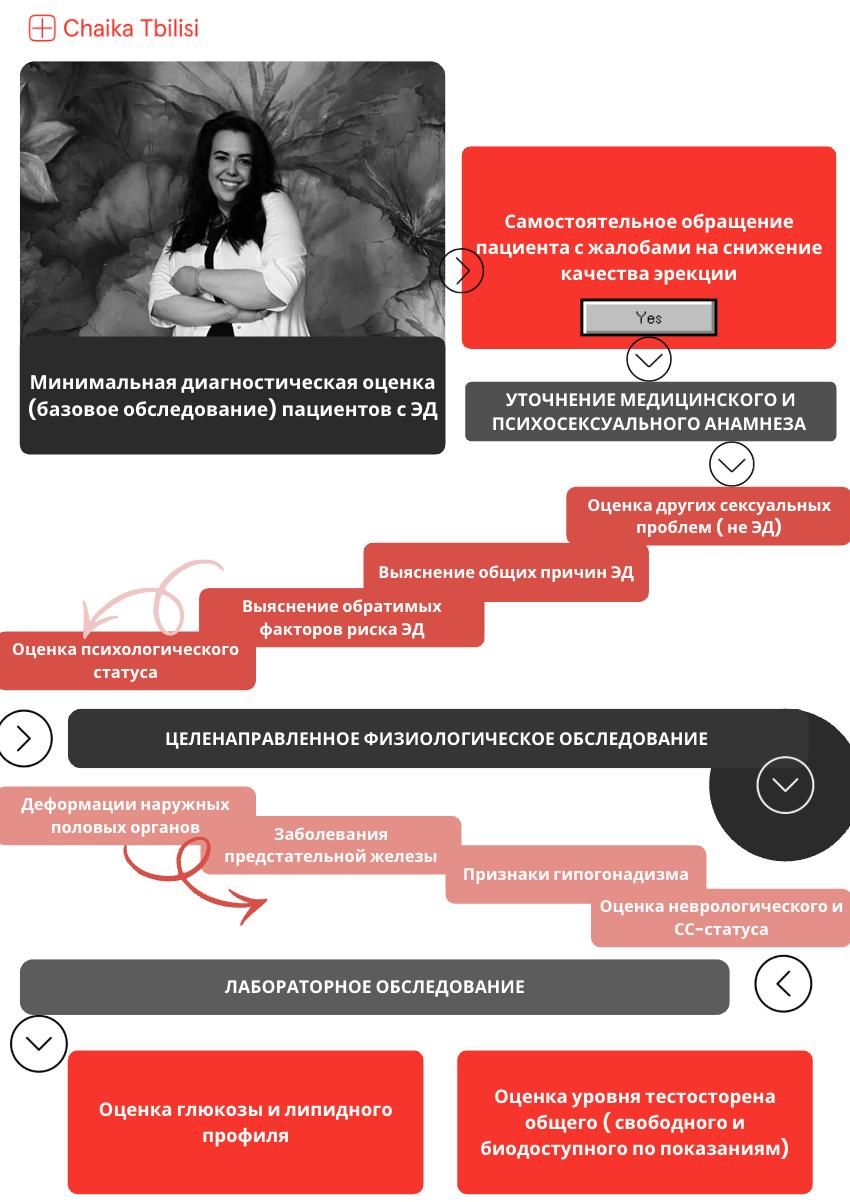
В отношении урологического здоровья причинами эректильной дисфункции могут быть совершенно разные заболевания и синдромы, включая симптомы нижних мочевыводящих путей и доброкачественную гиперплазию предстательной железы, синдром хронической тазовой боли (СХТБ) и хронический простатит [6], синдром болезненного мочевого пузыря /интерстициальный цистит [7], преждевременную эякуляцию [8] и уретропластику при стриктурах задней уретры.
Мужчины, обращающиеся к врачу по поводу нарушений эрекции, очень часто имеют скрытые или выявленные сердечно-сосудистые заболевания (ССЗ). Исследования показали, что ЭД существенно повышает риск развития ишемической болезни сердца, инсульта, фибрилляции предсердий, а также риск смерти от сердечно-сосудистых причин и общую смертность [9]. Особенно важен тот факт, что у мужчин моложе 50 лет даже временные проблемы с эрекцией могут быть ранним признаком повышенного сердечного риска [10].
Это означает, что эректильная дисфункция нередко выступает самым ранним предиктором сердечно-сосудистых заболеваний — часто раньше, чем появляются боли в груди или выявляются изменения на ЭКГ. Более выраженная и длительная ЭД обычно указывает на более высокий сердечно-сосудистый риск, а сама по себе она повышает точность скрининга скрытых ССЗ [11].
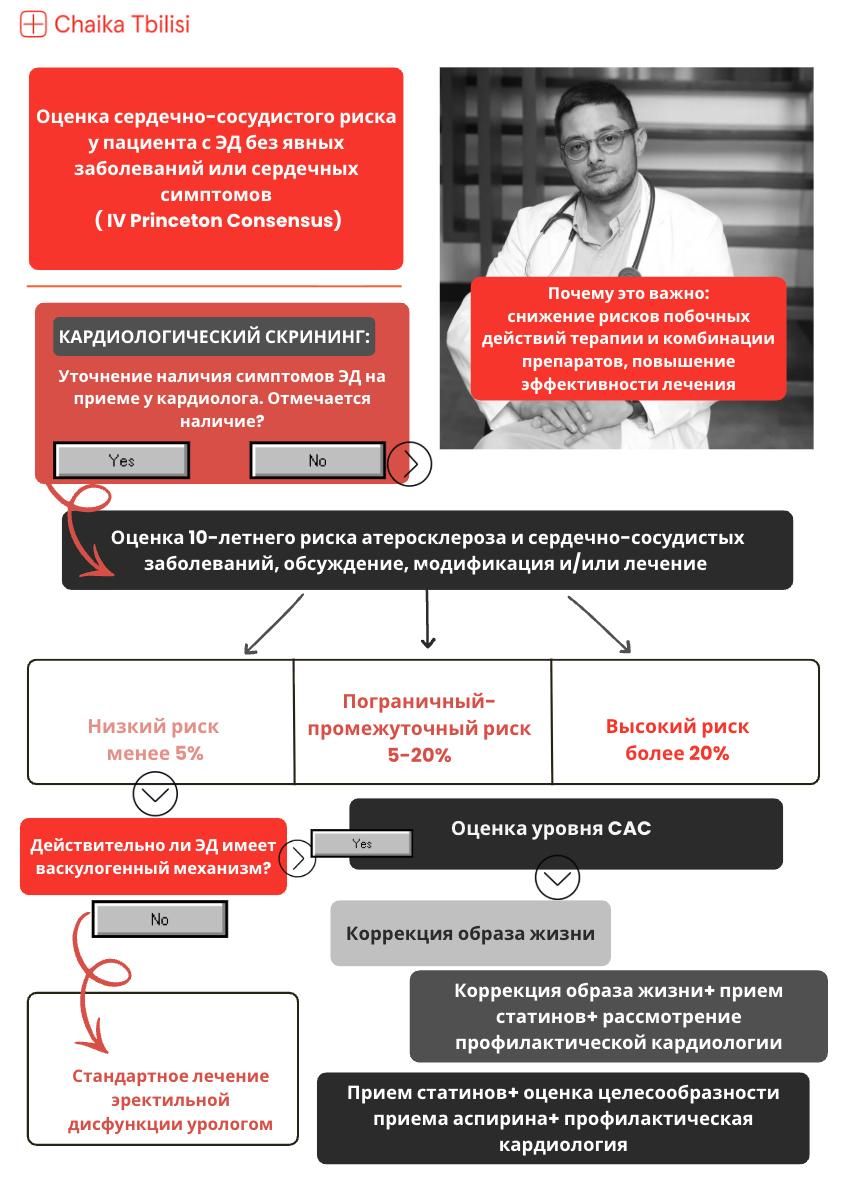
Серия конференций The Princeton Consensus была посвящена именно тому, как максимально эффективно и безопасно обследовать и лечить мужчин с ЭД и возможными сердечно-сосудистыми рисками [12]. Современные европейские рекомендации по эректильной дисфункции (EAU) основаны на последней версии Princeton Consensus, опубликованной в 2024 году [13].
IV четвёртая конференция Princeton Consensus пересмотрела алгоритмы оценки сердечного риска у мужчин с ЭД и рекомендовала использовать универсальный ASCVD-скор (American College of Cardiology/American Heart Association) для оценки 10-летнего риска крупных сердечно-сосудистых событий [14]. Этот расчёт учитывает возраст, пол, уровень холестерина, артериальное давление, курение и диабет после консультации врача-кардиолога
Обновлённые алгоритмы Princeton позволяют врачу определить:
насколько безопасна сексуальная активность при наличии ССЗ;
нужен ли углублённый кардиологический скрининг;
можно ли назначать препараты типа ингибиторов ФДЭ-5 (например, силденафил), особенно если пациент иногда использует нитраты
Эректильная дисфункция и психика: когда эмоции влияют на тело?
Проблемы с психическим здоровьем очень часто сопровождают эректильную дисфункцию (ЭД). [15]. Наиболее частыми психическими факторами выступают депрессия и тревожные расстройства, но нередко причинами становятся и временные эмоциональные кризисы — стресс на работе, семейные конфликты, утрата, переутомление. [16,17]
Эмоциональная атмосфера в отношениях играет огромную роль. Недовольство партнёрством, снижение сексуальной гармонии, длительность отношений, отсутствие эмоциональной близости во время секса — всё это повышает риск развития ЭД. Напротив, доверие и чувство поддержки со стороны партнёра выступают защитным фактором: мужчины, чувствующие эмоциональную безопасность в отношениях, гораздо реже сталкиваются с выраженными нарушениями эрекции. [16].
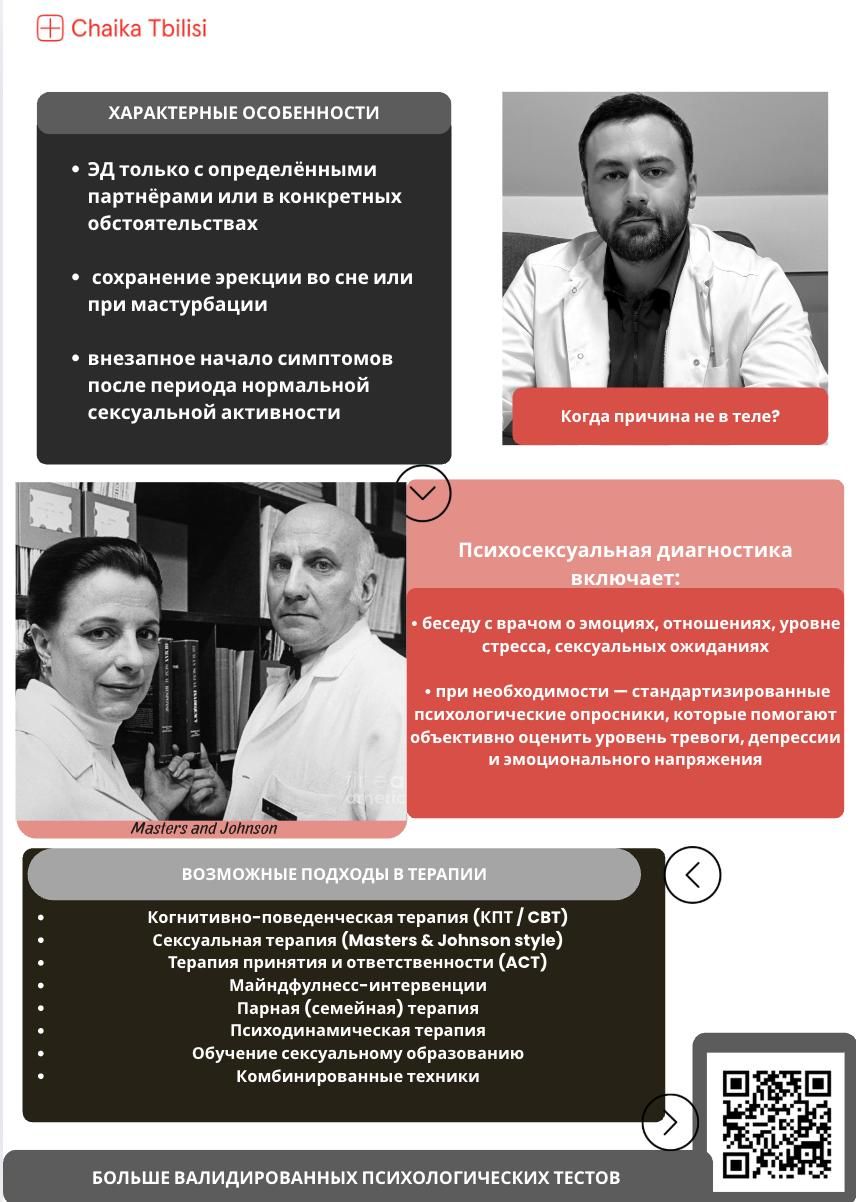
Когда причина не в теле?
Психогенная эректильная дисфункция — это форма нарушения эрекции, возникающая преимущественно из-за психологических факторов при возможной сохранности физиологических механизмов сексуальной функции.
В отличие от органической ЭД, при психогенной форме способность к эрекции сохраняется в ситуациях, когда половой акт невозможен или не предполагается. [17].
Характерными признаками являются:
эректильные трудности только с определёнными партнёрами или в конкретных обстоятельствах;
• сохранение эрекции во сне или при мастурбации;
• внезапное начало симптомов после периода нормальной сексуальной активности.
Эти особенности позволяют врачу предположить, что основная причина кроется не в теле, а в эмоциональной сфере [18,19].
Синдром ожидания неудачи
Одним из ключевых психологических механизмов, поддерживающих ЭД, является синдром ожидания неудачи. После пережитого неудачного опыта мужчина начинает тревожиться перед половым актом, что усиливает напряжение и снижает качество эрекции.
Типичные проявления включают:
• страх преждевременной эякуляции;
• опасение невозможности достижения оргазма;
• страх потери эрекции во время близости.
Такая тревога формирует замкнутый круг: чем сильнее страх неудачи, тем выше вероятность её повторения.
Почему важна психосексуальная диагностика?
Даже при «органической» эректильной дисфункции (например, вызванной сосудистыми нарушениями или действием лекарств) в процесс часто вовлечены когнитивные и эмоциональные факторы.
Негативные установки, чрезмерный самоконтроль, заниженная самооценка или отвлечение от эротических стимулов могут значительно усиливать проблему.
Поэтому врачу важно оценивать как физическое, так и психологическое состояние пациента.
Психосексуальная диагностика включает:
• беседу с врачом о эмоциях, отношениях, уровне стресса, сексуальных ожиданиях;
• при необходимости — стандартизированные психологические опросники, которые помогают объективно оценить уровень тревоги, депрессии и эмоционального напряжения.
Многогранная природа эректильной дисфункции.
Эректильная дисфункция почти никогда не имеет одной причины. У одного пациента могут сочетаться сосудистые, гормональные и неврологические нарушения, влияние лекарств, стресс и проблемы в отношениях [20].
По этой причине ЭД сегодня рассматривается как интегральный показатель мужского здоровья, отражающий как физическое, так и психологическое состояние.
Эффективное лечение требует комплексного подхода — участия уролога, кардиолога, психотерапевта и при необходимости эндокринолога.
Главное — помнить: даже при выраженных нарушениях эрекция часто восстанавливается, если вовремя обратиться за профессиональной помощью.
Источники отредачены
NIH, C.D.P.o.I. NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA, 1993. 270: 83.
- Feldman, H.A., et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol, 1994. 151: 54.
-Fisher, W.A., et al. Erectile dysfunction (ED) is a shared sexual concern of couples I: couple conceptions of ED. J Sex Med, 2009. 6: 2746.
-Salonia, A., et al. Is erectile dysfunction a reliable proxy of general male health status? The case for the International Index of Erectile Function-Erectile Function domain. J Sex Med, 2012. 9: 2708.
- Corona, G., et al. Assessment of the relational factor in male patients consulting for sexual dysfunction: the concept of couple sexual dysfunction. J Androl, 2006. 27: 795.
-Feldman, H.A., et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol, 1994. 151: 54.
-Braun, M., et al. Epidemiology of erectile dysfunction: results of the 'Cologne Male Survey'. Int J Impot Res, 2000. 12: 305.
-Wright, L.N., et al. Erectile Dysfunction and Treatment: An Analysis of Associated Chronic Health Conditions. Urology, 2021. 157: 148.
Li, H.J., et al. Prevalence of sexual dysfunction in men with chronic prostatitis/chronic pelvic pain syndrome: a meta-analysis. World J Urol, 2016. 34: 1009.
Chung, S.D., et al. A nationwide population-based study on bladder pain syndrome/interstitial cystitis and ED. Int J Impot Res, 2013. 25: 224.
.van der Poel, H.G., et al. Focal Therapy in Primary Localised Prostate Cancer: The European Association of Urology Position in 2018. Eur Urol, 2018. 74: 84.
- Tanaka, Y., et al. Association of Erectile Dysfunction with Incident Atrial Fibrillation: The Multi-Ethnic Study of Atherosclerosis (MESA). Am J Med, 2020. 133: 613.
Fang, S.C., et al. Changes in erectile dysfunction over time in relation to Framingham cardiovascular risk in the Boston Area Community Health (BACH) Survey. J Sex Med, 2015. 12: 100.
Adam, A., et al. Is the History of Erectile Dysfunction a Reliable Risk Factor for New Onset Acute Myocardial Infarction? A Systematic Review and Meta-Analysis. Curr Urol, 2020. 14: 122.
Rosen, R.C., et al. Proceedings of PRINCETON IV: PDE5 inhibitors and cardiac health symposium. Sex Med Rev, 2024. 12: 681.
Kloner, R.A., et al. Princeton IV consensus guidelines: PDE5 inhibitors and cardiac health. J Sex Med, 2024. 21: 90.
Reiter-Brennan, C., et al. ACC/AHA lipid guidelines: Personalized care to prevent cardiovascular disease. Cleve Clin J Med, 2020. 87: 231.
Li, K., et al. The Relationships of Dehydroepiandrosterone Sulfate, Erectile Function and General Psychological Health. Sex Med, 2021. 9: 100386.
Liu, Q., et al. Erectile Dysfunction and Depression: A Systematic Review and Meta-Analysis. J Sex Med, 2018. 15: 1073.
Rosen, R.C., et al. Men with Sexual Problems and Their Partners: Findings from the International Survey of Relationships. Arch Sex Behav, 2016. 45: 159.
Sivaratnam, L., et al. Behavior-Related Erectile Dysfunction: A Systematic Review and Meta-Analysis. J Sex Med, 2021. 18: 121.
Brotto, L., et al. Psychological and Interpersonal Dimensions of Sexual Function and Dysfunction. J Sex Med, 2016. 13: 538.
Parent, M.C., et al. Heterosexual Self-Presentation, Identity Management, and Sexual Functioning Among Men Who Have Sex with Men. Arch Sex Behav, 2021. 50: 3155.