Cholesterol After Age 19: Why Should Young People Check Their Lipids Too?
When we talk about cholesterol, many people still think of it as a problem of older age. It seems that high cholesterol is something that happens “after 50,” when a person already has high blood pressure, excess weight, diabetes, or previous cardiovascular events. There is also another common misconception: thinking that if a person eats normally, does not eat fast food, chips, sweets, does not drink carbonated beverages, and generally tries to live a healthy lifestyle, then they cannot have problems with cholesterol. Unfortunately, this is not always true. Cholesterol depends not only on diet. Heredity, metabolism, age, comorbidities, level of physical activity, and individual characteristics of the body also play a major role.
Modern cardiology takes a much broader view of this issue.
Today we understand that atherosclerosis does not appear suddenly. A heart attack, stroke, coronary artery stenosis, or the need for stent implantation is often the final stage of a process that may have started 10, 20, or even 30 years before the first symptoms. That is why modern guidelines increasingly emphasize early detection of lipid metabolism disorders.
What Is a Lipid Profile?
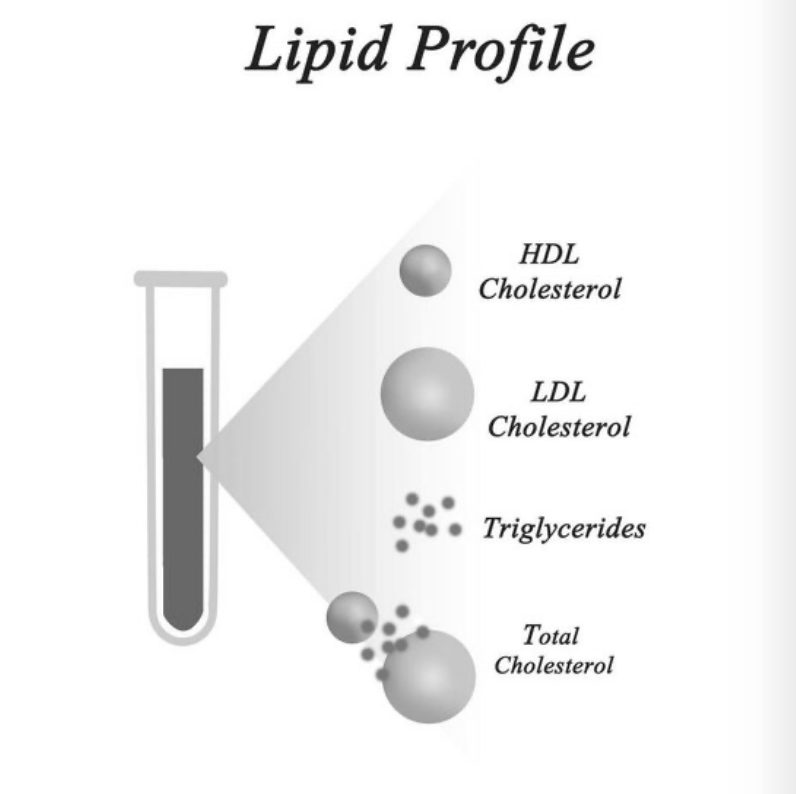
A lipid profile is a blood test that helps assess fat metabolism and the risk of developing atherosclerosis. It usually includes total cholesterol, low-density lipoproteins, high-density lipoproteins, triglycerides, and non-HDL cholesterol. In certain situations, a physician may recommend additional tests that help assess individual cardiovascular risk more accurately.
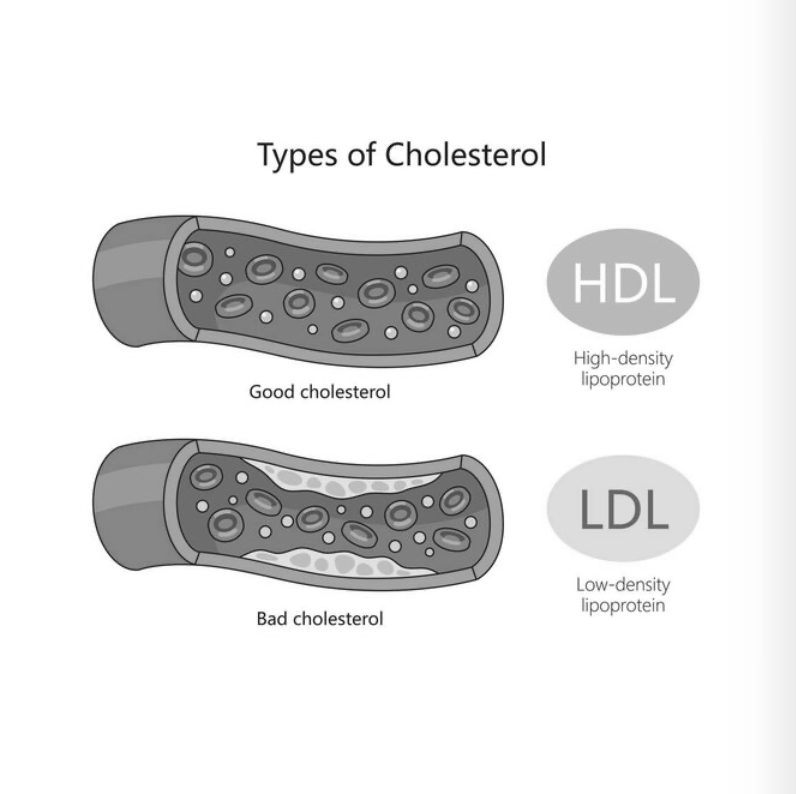
The best-known marker is LDL, or low-density lipoprotein. In everyday language, it is often called “bad cholesterol,” although it is more accurate to say that LDL is the main carrier of cholesterol involved in the formation of atherosclerotic plaques in the arteries. The higher the LDL level and the longer it remains elevated, the greater the cumulative burden on the vascular wall over a lifetime.
One of the key ideas of modern preventive cardiology is simple: it is important not only to lower cholesterol, but also to do it in time. The earlier an increased risk is identified and the longer lipids remain under control, the greater the chance of preventing serious cardiovascular events in the future.
Why Should Cholesterol Be Checked From a Young Age?
Modern American dyslipidemia guidelines emphasize that adults are recommended to check their lipid profile starting at approximately age 19, and then at least once every 5 years if the results are normal and there are no additional risk factors.
In practice, this is a very important point. Young people often have no complaints. Blood pressure may be normal, physical fitness may be good, body weight may be normal, and yet cholesterol may still be elevated. This is especially common in people with hereditary predisposition.
A person may be young, active, a non-smoker, physically fit, eat well, and still have high cholesterol because of genetics. In such cases, diet and physical activity are important, but sometimes they are not enough, because the problem is not only lifestyle but also the individual features of lipid metabolism.
Therefore, the phrase “I am young, it is too early for me to think about cholesterol” no longer works today. It is more accurate to say: the earlier we know our lipid profile, the more time we have to prevent disease rather than treat its consequences.
When Should Lipids Be Checked More Often Than Every 5 Years?
Once every 5 years is a general reference point for young people from age 19 who have no known lipid metabolism disorders and no major risk factors. But there are situations in which testing is needed earlier and more often.
For example, if close relatives had early heart attacks, strokes, stenting, or bypass surgery; if parents, brothers, or sisters had high cholesterol; if the person has already had lipid profile abnormalities; if there is arterial hypertension, diabetes, obesity, chronic kidney disease, smoking, autoimmune disease, or other risk factors.
It is also important to remember inherited lipid metabolism disorders. These are situations in which cholesterol may be significantly elevated from a young age. The danger is that a person may feel completely well for years, while the blood vessels are already exposed to an increased atherogenic burden.
In such cases, it is important to assess not only one blood test, but also family history, age, associated risk factors, and the overall clinical picture.
Cholesterol Is Not Just a Number in a Blood Test
One common mistake is looking at cholesterol in isolation. Many people try to understand “how bad it is” based only on one number in a blood test. But in real clinical practice, this approach is not correct.
The same value may mean completely different things for different people. For one person, it may be a reason to start with dietary changes, physical activity, weight reduction, and follow-up testing. For another person, it may already be an argument in favor of medication therapy, especially if there is a family history of early cardiovascular disease, diabetes, chronic kidney disease, signs of atherosclerosis, or high calculated risk.
Modern cardiology evaluates not only cholesterol, but overall cardiovascular risk: age, sex, blood pressure, smoking, presence of diabetes, kidney function, family history, lifestyle, comorbidities, and other parameters. That is why two people with similar test results may receive different recommendations. Conversely, an apparently healthy young person without symptoms may sometimes have a higher long-term risk than it seems at first glance.
What Is PREVENT and Why Is It Important?
In newer American approaches, the PREVENT calculator is being used increasingly often. It is a modern risk assessment model developed by the American Heart Association. It helps assess not only the near-term risk, but also the longer-term cardiovascular risk in adults.
This is especially important for young and relatively young people. In a person aged 30 to 40, the short-term risk often looks low simply because the person is young. But when looking at the long-term perspective, the picture may be very different.
For example, a person may have a low probability of a cardiovascular event in the next few years, but at the same time have a high long-term risk due to elevated cholesterol, high blood pressure, smoking, family history, or other factors. And it is precisely at this age that prevention may have the greatest effect.
Simply put, PREVENT helps us avoid waiting until the risk becomes obviously high and allows us to identify the problem earlier.
When Are Lifestyle Changes Alone Not Enough?
Healthy eating, regular physical activity, weight control, smoking cessation, and normal sleep are the foundation of prevention. But it is important to be honest: not every case of high cholesterol can be “eaten away” by diet. If cholesterol is significantly elevated, if there is hereditary predisposition, if there are already signs of atherosclerosis, or if cardiovascular risk is high, a physician may recommend medication therapy. The basis of treatment is often drugs that lower atherogenic lipid levels and reduce the risk of heart attack, stroke, and progression of atherosclerosis.
The goal of treatment is not to “put a person on pills.” The goal is to reduce the risk of serious events in the future. It is important to understand that therapy is selected individually. There is no single universal regimen for everyone. The decision depends on the lipid profile, overall risk, age, comorbidities, drug tolerability, family history, and treatment goals.
Main Message
Cholesterol is not just a blood test. It is one of the key factors that determines the condition of the blood vessels for decades ahead.
There is no need to wait for chest pain, shortness of breath, high blood pressure, or an incidental finding during an examination. Checking a lipid profile is simple. Correctly interpreting it is already the physician’s task. It is especially important to seek consultation if abnormalities have already been found in your blood tests, if there is a family history of early cardiovascular disease, if you are between 30 and 40 years old and want to understand your real risk, or if you have hypertension, diabetes, excess weight, smoking, chronic kidney disease, or other risk factors.
Modern preventive cardiology makes it possible not simply to “treat cholesterol,” but to assess individual risk, determine targets, choose the right strategy, and prevent in time events that may change a person’s life.
Prevention is not fear of disease. It is competent management of your future.